
What Is Cardiac Arrest vs a Heart Attack?
So, What Is Cardiac Arrest vs a Heart Attack?
Cardiac arrest vs a heart attack is a comparison we see very frequently, but they are two very different medical emergencies. A heart attack is a circulation problem, caused by a blocked artery that stops blood reaching part of the heart muscle. A cardiac arrest is an electrical problem, where the heart suddenly stops pumping altogether and the person collapses. One is usually a conscious patient with chest pain who needs urgent hospital treatment. The other is an unconscious patient who needs immediate CPR and a defibrillator within minutes.
In our experience at our Tunbridge Wells clinic, this is one of the most common pieces of confusion patients raise during consultations, often after a relative or colleague has had one or the other. From working with patients across Kent and East Sussex since 2006 at West Kent Cardiology Partnership, we have found that understanding the difference matters for two practical reasons. Firstly, the emergency response is different. Secondly, the risk factors and prevention strategies overlap but are not identical, and knowing which event you or a family member is at higher risk of changes the conversation about screening and treatment.
What is a heart attack?
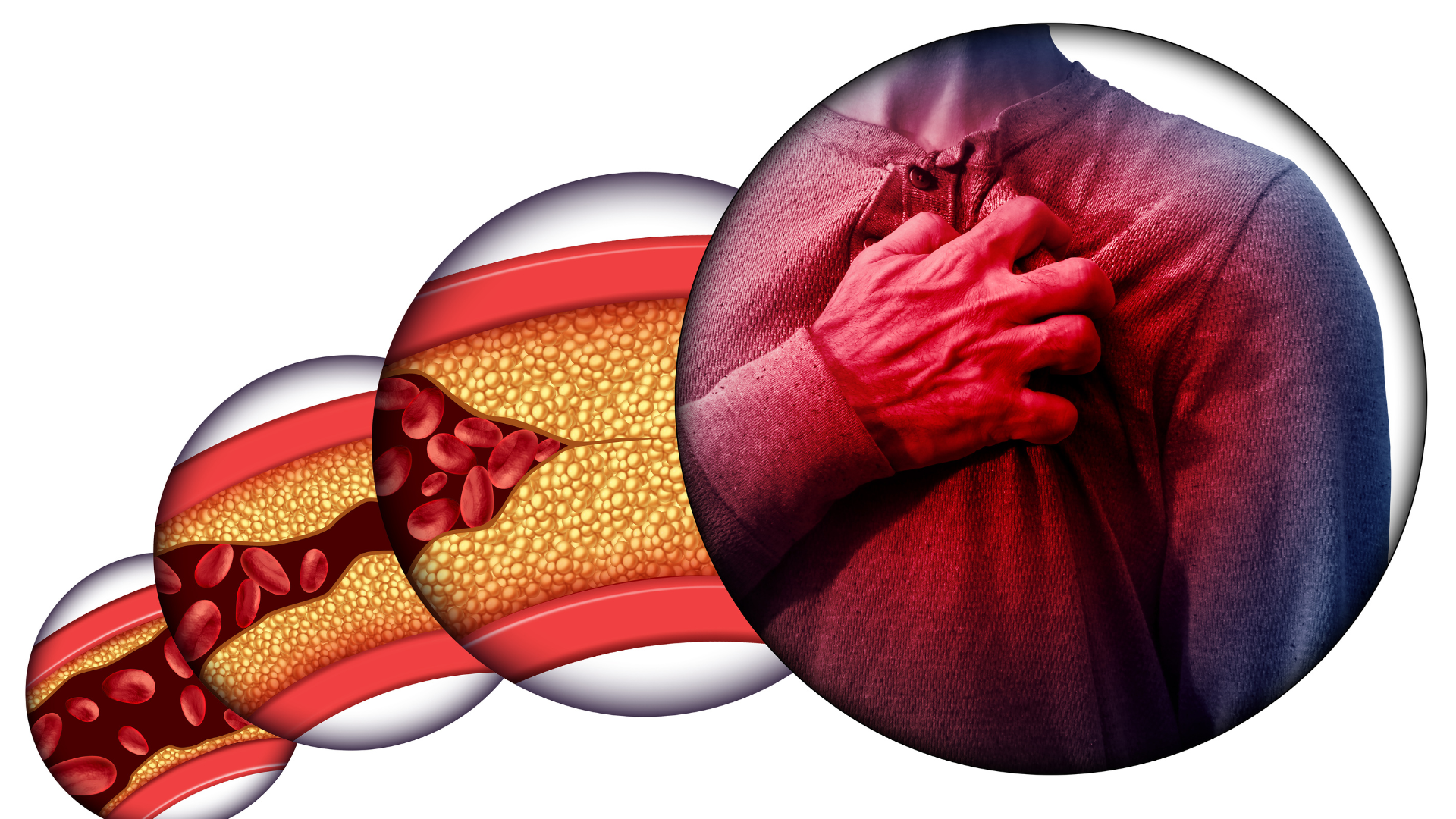
A heart attack happens when one of the coronary arteries supplying blood to the heart muscle becomes blocked, usually by a blood clot forming on top of fatty plaque that has built up over years. Without blood and oxygen, the affected area of heart muscle begins to die. The medical term is myocardial infarction.
The classic symptoms include chest pain or pressure that may feel like crushing, tightness, or heaviness, often spreading to the arm, jaw, neck, or back. Other features include sweating, breathlessness, nausea, light-headedness, and a sense that something is seriously wrong. Some people, particularly women, older adults, and those with diabetes, experience atypical symptoms such as nausea and fatigue without prominent chest pain.
Crucially, in a heart attack the person is usually still conscious. The heart is still beating, even if it is damaged. The treatment is to restore blood flow to the affected artery as quickly as possible, either with clot-busting medication or, more commonly, with emergency coronary angioplasty and stenting.
In our experience, the patients with the best outcomes from a heart attack are those who call 999 within the first hour of symptoms starting. From working with patients, we have found that the most common reason for delay is uncertainty about whether the symptoms are “bad enough”, particularly when chest pain is mild or feels like indigestion. In our experience, calling 999 at the first suspicion works better than waiting to see if symptoms settle, because every additional 30 minutes of delay allows more heart muscle to die.
What is a cardiac arrest?
A cardiac arrest is when the heart suddenly stops pumping blood around the body. The person collapses without warning, loses consciousness immediately, and stops breathing normally. Without intervention within minutes, the person will die. This is the most extreme form of medical emergency.
A cardiac arrest is caused by a dangerous abnormal heart rhythm, most often ventricular fibrillation, where the heart’s electrical system fails and the heart muscle quivers chaotically instead of pumping. Because no blood is being pumped, the brain is starved of oxygen and damage begins within three to four minutes.
Treatment involves immediate CPR to keep blood and oxygen circulating manually, and defibrillation, an electrical shock delivered to the chest, to restart a coordinated rhythm. Survival drops by around 10% with every minute that passes without defibrillation, which is why public access defibrillators in places like train stations and gyms are so important.
In our experience, the single biggest predictor of surviving a cardiac arrest outside hospital is whether a bystander starts CPR before the ambulance arrives. From working with patients and their families, we have found that hands-only CPR, chest compressions without rescue breaths, is far more likely to be given by bystanders than full CPR, and the evidence shows it is highly effective. In our experience, encouraging family members to learn hands-only CPR works better than relying on professional response alone, because outside-hospital cardiac arrest survival in the UK still sits below one in ten without it.
The key differences at a glance
The simplest way to think about it: a heart attack is a plumbing problem. A cardiac arrest is an electrical problem.
In a heart attack, blood flow to part of the heart is blocked, the heart muscle is damaged, and the person is usually awake and in pain. In a cardiac arrest, the heart’s electrical system fails, the heart stops pumping, and the person collapses unconscious.
A heart attack can trigger a cardiac arrest, which is the most important link between the two. When a section of heart muscle is starved of oxygen during a heart attack, it can become electrically unstable and trigger a dangerous rhythm. This is why many out-of-hospital cardiac arrests in adults happen in the context of an underlying, sometimes unrecognised, heart attack.
A cardiac arrest, however, can also occur without a heart attack. Other causes include inherited heart conditions such as hypertrophic cardiomyopathy and long QT syndrome, severe heart failure, electrolyte disturbances, drug toxicity, and electrical conduction problems in the heart.
Recognising the warning signs
A heart attack often gives warning signs. These include chest pain or pressure that may be intermittent in the days or weeks beforehand, unusual breathlessness on exertion, new fatigue, jaw or arm discomfort, indigestion-like symptoms that do not respond to antacids, and pain that is brought on by exertion and eases with rest.
A cardiac arrest, by contrast, usually happens without warning. The person collapses suddenly, stops responding, and stops breathing or breathes in a gasping, abnormal way, sometimes called agonal breathing. There is no time to question what is happening. The response is to call 999 immediately and start chest compressions.
In our experience, around 1 in 4 patients who go on to have a cardiac arrest had some form of warning sign in the preceding month that was dismissed as something else, including unexplained chest discomfort, episodes of fainting, palpitations, or breathlessness. From working with patients, we have found that recognising these earlier symptoms and arranging timely cardiac assessment is one of the most effective things people can do to reduce the risk of a sudden cardiac event.
What to do in each emergency
For a suspected heart attack, call 999 immediately and tell the operator you suspect a heart attack. Sit the person down in a comfortable position, ideally on the floor with knees bent and back supported. If they are not allergic and have access to it, chew a 300mg aspirin tablet. Keep them calm and still until the ambulance arrives. Do not drive them to hospital yourself.
For a suspected cardiac arrest, call 999 immediately. Shout for someone to find the nearest defibrillator. Start chest compressions in the centre of the chest at a rate of around 100 to 120 per minute, the rhythm of “Stayin’ Alive” works well. Push hard and fast and do not stop until the ambulance arrives or a defibrillator is available. If a defibrillator is brought, switch it on and follow the spoken instructions.
Who is at risk?
The risk factors for a heart attack are largely the risk factors for coronary artery disease: high blood pressure, high cholesterol, diabetes, smoking, family history of heart disease, obesity, physical inactivity, and increasing age.
The risk factors for a cardiac arrest overlap with these, because most adult cardiac arrests happen against a background of coronary disease. However, additional risk factors include previous heart attack, heart failure with reduced pumping function, inherited heart rhythm conditions, certain cardiomyopathies, and a family history of sudden unexplained death under the age of 40.
From working with patients, we have found that a family history of sudden death in a young relative is one of the most overlooked risk factors. In our experience, families affected by an unexplained sudden death benefit significantly from early screening of first-degree relatives, because many of the underlying conditions are inherited and can be identified before they cause a problem.
How we assess risk
A baseline cardiac assessment is the best way to identify whether you are at increased risk of a heart attack or cardiac arrest before symptoms develop. Assessment usually starts with a detailed history including family history, an ECG to check rhythm and electrical conduction, blood tests including cholesterol and inflammatory markers, and an echocardiogram to look at heart structure and function.
Where there is concern about exertional symptoms, an exercise stress test or stress echo study helps reveal problems that only show up under load. A CT coronary angiogram provides direct imaging of the coronary arteries and is one of the most useful tests for assessing heart attack risk. For patients with palpitations or unexplained blackouts, a 24-hour ECG recording or 7-day cardiac event recorder can capture rhythm disturbances that point to cardiac arrest risk.
In our experience, a comprehensive baseline assessment such as our HeartScreen programme works better than waiting for symptoms in patients with significant risk factors or family history, because most of the people who go on to have a serious cardiac event had identifiable risk in the years beforehand. From working with patients, we have found that early identification typically allows risk to be managed with medication and lifestyle changes alone, without the need for procedures.
Reducing your risk
The same broad strategy reduces risk of both heart attack and cardiac arrest: keep blood pressure and cholesterol in a healthy range, manage diabetes carefully, stop smoking, maintain a healthy weight, exercise regularly, and limit alcohol. For people with established heart disease, taking prescribed medication consistently is one of the most important factors.
For patients identified as being at high risk of a dangerous heart rhythm, additional measures may be appropriate, including specific anti-arrhythmic medication or, in selected cases, an implantable defibrillator that can detect and treat a life-threatening rhythm automatically.
Conclusion
A heart attack and a cardiac arrest are both medical emergencies but they are not the same condition. A heart attack is a blocked artery causing damage to the heart muscle, with the person usually conscious and in pain. A cardiac arrest is the heart’s electrical system failing, with the person unconscious and not breathing. A heart attack can lead to a cardiac arrest, but a cardiac arrest can also happen without one. The emergency response is different, and so is the longer-term management of risk.
If you have risk factors for heart disease, a family history of cardiac events, or symptoms that worry you, the most effective step you can take is to have a proper baseline cardiac assessment before a problem develops. You can contact us, Dr Clive Lawson and Dr Derek Harrington at West Kent Cardiology Partnership, to arrange an assessment at our Tunbridge Wells clinic, or call us directly on 01892 526726.